Quick Takeaways
- Most hiccups are short‑lived and harmless, but persistent episodes can signal a deeper issue.
- Swallowing disorders (dysphagia) often share nerve or muscle pathways with hiccups.
- Key triggers include gastro‑esophageal reflux, certain medications, and neurological conditions.
- Early diagnosis relies on a focused history, simple bedside tests, and, when needed, imaging.
- Treatment ranges from lifestyle tweaks to targeted therapies like biofeedback or medication.
What Hiccups actually are?
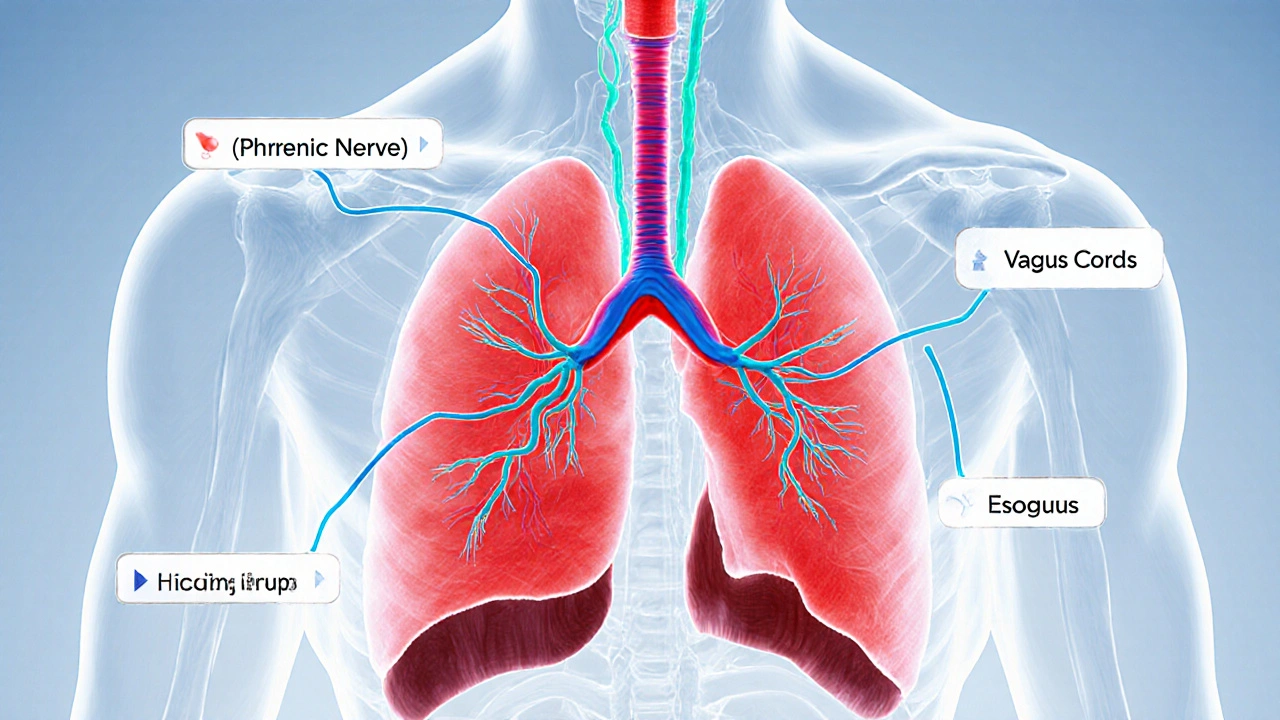
When you get hiccups, your diaphragm the large muscle beneath the lungs that drives breathing contracts suddenly. The vocal cords snap shut, creating the classic "hic" sound. In most people the episode lasts a few minutes and resolves on its own.
Although the exact trigger loop isn’t fully mapped, the reflex arc involves the vagus nerve a cranial nerve that carries sensory information from the throat, abdomen, and heart to the brain. Anything that irritates the vagus or the phrenic nerve (which directly innervates the diaphragm) can set off the hiccup cycle.
When hiccups intersect with swallowing problems
Swallowing disorders are medically termed dysphagia difficulty moving food or liquid from the mouth to the stomach. Because both hiccups and dysphagia rely on overlapping nerve pathways-primarily the vagus and the glossopharyngeal nerves-persistent hiccups can be a red flag for an underlying swallowing issue.
Common scenarios include:
- Acid reflux that irritates the esophagus and the vagus nerve.
- Neurological diseases such as Parkinson’s or multiple sclerosis that disrupt nerve signaling.
- Structural blockages (tumors, strictures) that force the airway to overcompensate.

Top causes of chronic hiccups and dysphagia
Understanding the root triggers helps you target the right treatment. Below are the most frequent culprits, grouped by system.
| Feature | Acute (≤48 hrs) | Persistent (>48 hrs) / Intractable (>1 month) |
|---|---|---|
| Typical triggers | Fast eating, carbonated drinks, sudden temperature change | GERD, central nervous system lesions, medication side effects |
| Associated symptoms | None or mild bloating | Chest pain, weight loss, coughing, difficulty swallowing |
| First‑line management | Home remedies (holding breath, sipping water) | Medical evaluation, imaging, targeted therapy |
Beyond reflux, several medication side effects are notorious for inducing hiccups-especially steroids, benzodiazepines, and some chemotherapy agents. Likewise, certain drugs (anticholinergics, sedatives) can thin the muscle coordination needed for safe swallowing, leading to dysphagia.
Neurological conditions deserve a special mention. Parkinson’s disease often causes both stiff muscles and impaired reflexes, making hiccups and swallowing difficulties a common combo. In multiple sclerosis, demyelination of the vagus pathway can spark similar symptoms.
How doctors diagnose the link
When you present with hiccups that last more than 48 hours, clinicians typically start with a thorough history:
- Duration and pattern of hiccups (continuous, intermittent, triggered by food).
- Associated swallowing complaints (coughing after meals, sensation of food sticking).
- Medication list and recent changes.
- Presence of reflux symptoms or known neurological disease.
Physical exam focuses on the neck, throat, and respiratory sounds. Simple bedside tests include the “water swallow test” (patient drinks a cup of water; the clinician watches for coughing or throat clearing) and a “tongue‑pressure test” to gauge muscle strength.
If red flags appear-weight loss, unexplained pain, or neurological deficits-further studies are ordered:
- Upper endoscopy to look for esophageal inflammation or strictures.
- Videofluoroscopic swallow study (VFSS) to visualize the swallowing process in real time.
- Brain MRI when a central cause is suspected.
- Blood tests for metabolic imbalances (e.g., hyponatremia) that can precipitate hiccups.
Treatment pathways - from home tricks to medical interventions
Therapy is tiered based on severity.
Self‑care and lifestyle tweaks
- Eat slowly, chew thoroughly, and avoid carbonated beverages.
- Elevate the head of the bed 10‑15cm to reduce nighttime reflux.
- Maintain a healthy weight; excess abdominal pressure can aggravate the diaphragm.
- Try proven home tricks: sip cold water, swallow a teaspoon of sugar, or gently pull on the tongue.
Medication options
When hiccups persist, doctors may prescribe:
- Chlorpromazine - a dopamine blocker shown to calm the hiccup reflex in up to 70% of cases.
- Metoclopramide - helps both reflux and hiccups by enhancing gastric emptying.
- Low‑dose gabapentin for neuropathic hiccups linked to nerve irritation.
For dysphagia, treatment targets the root cause:
- Proton‑pump inhibitors (PPIs) for GERD‑related swallowing difficulty.
- Swallowing therapy with a speech‑language pathologist.
- Botulinum toxin injections for focal muscle spasm.
Advanced therapies
Biofeedback therapy uses visual or auditory cues to help patients regain control of muscle coordination has shown promise for chronic hiccups tied to nerve misfiring. It works by training the patient to modulate diaphragmatic activity through real‑time monitoring.
In rare cases where a tumor or structural lesion is the culprit, surgical removal or endoscopic dilation may be necessary.
Practical tips to keep hiccups and swallowing issues at bay
- Keep a food diary for a week; note any patterns between meals and hiccup episodes.
- Avoid tight clothing around the abdomen, especially after meals.
- Stay hydrated, but sip water rather than gulp large volumes.
- If you take steroids, discuss tapering schedules with your doctor to minimize side effects.
- Schedule regular dental and ENT check‑ups; oral infections can trigger vagus irritation.

When to seek professional help
While most hiccups disappear on their own, you should call a healthcare provider if any of the following occur:
- Hiccups last longer than 48hours.
- You notice coughing, choking, or a feeling that food is stuck.
- Weight loss, persistent heartburn, or night‑time regurgitation develop.
- Neurological symptoms appear-tremor, slurred speech, or loss of balance.
- Medications have recently changed and symptoms began shortly after.
Early assessment can prevent complications like aspiration pneumonia, malnutrition, or chronic gastro‑esophageal damage.
Frequently Asked Questions
Can stress cause hiccups?
Yes. Stress can trigger the vagus nerve, leading to brief hiccup bouts. Managing anxiety with breathing exercises often helps reduce episodes.
Is dysphagia always a sign of a serious disease?
Not always. Many people have mild swallowing difficulty from reflux or a recent cold. However, persistent dysphagia warrants a medical check‑up to rule out deeper issues.
What home remedy works best for a hiccup bout?
Sipping a glass of cold water while holding your breath for about 10 seconds is one of the most reliable tricks. The combination resets the diaphragm’s rhythm.
Can certain foods make hiccups worse?
Spicy, very hot, or carbonated foods can irritate the esophagus and trigger the vagus nerve, extending hiccup episodes.
Are there any long‑term complications from chronic hiccups?
If left untreated, chronic hiccups can lead to fatigue, weight loss, sleep disruption, and even esophageal tears from repeated forceful contractions.

Comments (11)
Rohinii Pradhan
Your exposition on the pathophysiology of hiccups is commendably comprehensive, yet it neglects to acknowledge the pivotal role of the phrenic nerve in diaphragmatic spasms.
A nuanced understanding of vagal afferents should be accompanied by a thorough discussion of the cervical plexus contributions.
Moreover, the table you present suffers from typographical inconsistencies that could confound the discerning reader.
While the therapeutic section is exhaustive, the omission of baclofen as a potential antispasmodic is a glaring oversight.
In sum, the article is informative but would benefit from a more rigorous editorial polish.
Anna-Lisa Hagley
The article equates hiccups with a mere nuisance, ignoring their existential symbolism as involuntary rebellions of the body.
One could argue that the true ailment lies not in the diaphragm but in the mind's futile quest for control.
Consequently, the medical approach appears superficial.
A Walton Smith
Looks like a copy‑paste job.
Alisa Hayes
I appreciate the effort to collate the basics, but the flow could use a bit more structure.
For instance, linking the reflux discussion directly to the swallowing tests would clarify the clinical pathway.
Also, a brief summary at the end might help readers synthesize the key takeaways.
Mariana L Figueroa
Great overview! If you’re dealing with persistent hiccups, try a daily probiotic; it can reduce reflux triggers.
Also, consider a gentle diaphragmatic breathing routine before meals to stabilize the reflex.
For dysphagia, a short session with a speech‑language therapist can make a huge difference.
mausumi priyadarshini
While your suggestions are well‑intentioned, one must question their universal applicability; not everyone tolerates probiotics, and excessive emphasis on breathing exercises may overlook underlying neuropathic causes, which demand a more comprehensive neurological assessment; moreover, the assumption that a brief therapy session suffices seems overly optimistic.
Thus, a balanced approach that integrates dietary, pharmacological, and neurophysiological strategies would be more prudent.
Carl Mitchel
It is morally incumbent upon clinicians to address chronic hiccups promptly, lest patients endure preventable suffering.
Ignoring the psychosocial impact of incessant spasms is tantamount to negligence.
Furthermore, prescribing chlorpromazine without assessing potential side effects violates the principle of informed consent.
A holistic treatment plan, incorporating lifestyle modification, mental health support, and judicious pharmacotherapy, aligns with ethical best practice.
Empathy should accompany every diagnostic step, because the burden of dysphagia extends beyond the esophagus into the patient's daily existence.
Suzette Muller
I hear your concern for patient welfare, and I agree that compassion is essential.
In my experience, offering a simple food diary early on can empower patients to identify trigger patterns.
Coupling this with a gentle education session about posture during meals often yields noticeable improvement.
Remember, small supportive gestures can make a big difference in the healing journey.
Josh SEBRING
Honestly, none of this fancy jargon matters if you’re just trying to stop a hiccup at the dinner table.
Who needs an MRI when a spoonful of sugar does the trick?
Stop overcomplicating a simple reflex and just breathe.
Lily Tung
The phenomenon of hiccups, though often dismissed as trivial, warrants a thorough scientific investigation.
Recent studies have elucidated the complex interplay between the vagus nerve and the central respiratory centers.
A detailed analysis reveals that neurotransmitter imbalances can precipitate persistent diaphragmatic contractions.
Moreover, the gastrointestinal microbiome exerts a subtle yet significant influence on esophageal sensitivity.
Clinical observations indicate that patients with chronic reflux frequently exhibit heightened hiccup frequency.
Therapeutic interventions therefore must address both the upper gastrointestinal tract and neural pathways.
Pharmacological options such as chlorpromazine have demonstrated efficacy in attenuating refractory episodes.
Nevertheless, clinicians should remain vigilant regarding potential adverse effects including hypotension and sedation.
Non‑pharmacologic techniques, for example, diaphragmatic breathing and biofeedback, serve as valuable adjuncts.
In addition, dietary modifications that reduce carbonated beverage consumption can mitigate trigger exposure.
Patient education regarding posture and meal pacing further contributes to symptom reduction.
When suspecting an underlying structural anomaly, endoscopic evaluation remains the gold standard diagnostic tool.
Conversely, in the absence of red‑flag signs, a conservative approach centered on lifestyle alteration is appropriate.
Future research should aim to delineate the molecular mechanisms governing the hiccup reflex arc.
Such insights may pave the way for targeted therapies with improved safety profiles.
In summary, a multidisciplinary strategy integrating medical, behavioral, and nutritional components optimizes patient outcomes.
Taryn Bader
I guess some people just love the drama of endless hiccups.