Understanding Diabetic Gastroparesis
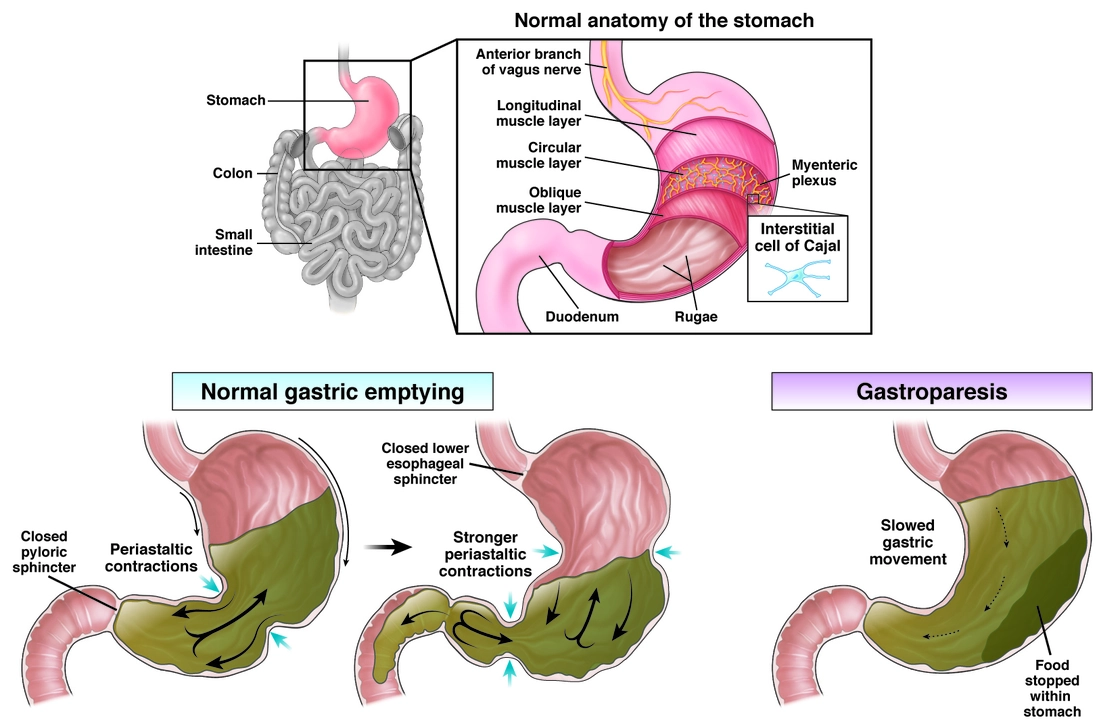
Before diving into the potential role of Domperidone in treating diabetic gastroparesis, it is essential to understand what diabetic gastroparesis is and how it affects patients. Gastroparesis is a condition characterized by delayed gastric emptying, leading to symptoms such as nausea, vomiting, abdominal pain, and bloating. In diabetic patients, gastroparesis occurs due to nerve damage caused by high blood sugar levels, which affects the normal functioning of the stomach muscles.
This condition can significantly impact a patient's quality of life, leading to malnutrition, dehydration, and severe fluctuations in blood sugar levels. It is crucial to find effective treatment options to manage the symptoms and improve the overall health of patients suffering from diabetic gastroparesis.
Introduction to Domperidone
Domperidone is an oral medication primarily used to treat nausea and vomiting. It belongs to the class of drugs called dopamine antagonists, which work by blocking the action of dopamine in the brain. Dopamine is a neurotransmitter that has various functions, including regulating the movement of food through the gastrointestinal tract.
By blocking the action of dopamine, Domperidone enhances the contractions of the stomach muscles, thus promoting gastric emptying and reducing the symptoms associated with gastroparesis. Domperidone is not currently approved for use in the United States but is available in various other countries for the treatment of gastrointestinal disorders.
Domperidone and Diabetic Gastroparesis: A Promising Option
Several studies have been conducted to explore the potential role of Domperidone in treating diabetic gastroparesis. Overall, the results have been promising, with most studies showing a significant improvement in gastric emptying and a reduction in the severity of symptoms.
One study conducted on patients with diabetic gastroparesis found that Domperidone significantly improved gastric emptying and reduced vomiting episodes in comparison to a placebo group. Another study reported similar results, with Domperidone proving to be more effective than other prokinetic agents in improving gastric emptying and reducing gastroparesis symptoms. These findings suggest that Domperidone may be a valuable treatment option for patients with diabetic gastroparesis.
Comparing Domperidone with Other Treatment Options
There are several other medications available for treating gastroparesis, including metoclopramide and erythromycin. However, these medications may have limitations and side effects that make them less suitable for some patients. For example, metoclopramide, another dopamine antagonist, has been associated with severe neurological side effects, such as tardive dyskinesia, a condition characterized by involuntary, repetitive movements.
On the other hand, erythromycin, an antibiotic, can lose its effectiveness over time as the body develops a tolerance to the drug. In comparison, Domperidone has been found to have a more favorable side effect profile and does not appear to cause the same neurological side effects as metoclopramide. Therefore, Domperidone may be a safer and more effective alternative for many patients with diabetic gastroparesis.
Domperidone Safety and Side Effects
While Domperidone has been found to have a more favorable side effect profile compared to other prokinetic agents, it is not entirely without risks. Some of the most common side effects associated with Domperidone include headache, dizziness, dry mouth, and gastrointestinal disturbances. These side effects are generally mild and tend to resolve with time.
However, there have been concerns about the potential for Domperidone to cause cardiac side effects, such as QT interval prolongation, which can lead to a potentially life-threatening arrhythmia called Torsades de Pointes. As a result, Domperidone is contraindicated in patients with existing heart conditions or those at risk for QT interval prolongation. It is essential for healthcare providers to carefully weigh the potential benefits and risks of Domperidone when considering it as a treatment option for diabetic gastroparesis.
Access to Domperidone for Diabetic Gastroparesis Patients
As mentioned earlier, Domperidone is not currently approved for use in the United States. However, it is available in other countries, such as Canada and the United Kingdom, where it is commonly prescribed for gastrointestinal disorders. For patients in the United States seeking access to Domperidone, the FDA has established an Investigational New Drug (IND) program that allows patients with severe gastroparesis symptoms to receive the medication under specific conditions and close medical supervision.
To access Domperidone through the IND program, patients must have a prescription from a healthcare provider who is registered with the program and must obtain the medication from a specially authorized pharmacy. While this process may be more complex than obtaining other medications, it may be worth considering for patients who have not found relief with other treatment options and believe Domperidone may help manage their diabetic gastroparesis symptoms.
Conclusion: A Potential Game Changer for Diabetic Gastroparesis Patients
Domperidone has shown promising results in the treatment of diabetic gastroparesis, with many studies demonstrating its effectiveness in improving gastric emptying and reducing symptoms. Its favorable side effect profile and fewer neurological side effects compared to other prokinetic agents make it an attractive option for many patients. However, it is essential to carefully consider the potential risks associated with Domperidone, particularly concerning cardiac side effects.
For patients in the United States, accessing Domperidone may be more challenging due to its unapproved status, but the FDA's IND program provides a pathway for those who believe the medication may help manage their symptoms. Ultimately, the potential role of Domperidone in treating diabetic gastroparesis should be discussed with a healthcare provider who can help determine the most appropriate treatment plan based on individual needs and circumstances.

Comments (15)
Zach Harrison
Domperidone is actually pretty cool if you can get it. I’ve been on it for my gastroparesis for two years now. No weird tics like with metoclopramide. Just less bloating and way fewer vomiting episodes. My doc had to jump through hoops to get it for me, but worth it.
M. Kyle Moseby
Why are we even talking about this drug? It’s banned in the US for a reason. People die from heart issues with this stuff. Stop pushing dangerous meds like they’re magic pills.
Terri-Anne Whitehouse
Interesting how the author cherry-picks studies from Canada and the UK while ignoring the EMA’s 2014 safety review that restricted domperidone to short-term use only. The data is *technically* promising, but the risk-benefit ratio remains deeply questionable. Also, why no mention of cisapride’s history? This feels like a nostalgia trip for outdated pharmacology.
Matthew Williams
Oh great, another article pushing foreign meds because Americans can’t handle real medicine. Metoclopramide works fine if you don’t take it for 5 years straight. And now we’re gonna import some sketchy European pill that got pulled because people started having heart attacks? This is why the US healthcare system is better - we don’t let you kill yourself with unapproved junk.
Dave Collins
Of course domperidone is ‘promising.’ It’s the only thing left that doesn’t make you twitch like a robot having a seizure. Meanwhile, the FDA is out here treating gastroparesis patients like lab rats while Big Pharma sells them $500/month ‘alternatives’ that do nothing. Bless their hearts.
Idolla Leboeuf
DO IT. If this helps even one person stop vomiting at 3am, it’s worth fighting for. Stop letting bureaucracy kill quality of life. I’m getting mine through the IND program - it’s not easy but it’s possible. You got this.
Cole Brown
Hey, I just wanted to say - if you’re considering domperidone, please talk to your doctor first. Make sure they check your EKG and know your full med history. I had a friend who didn’t and it didn’t end well. But if it’s right for you, it can be life-changing. Don’t give up.
Danny Pohflepp
Let’s not ignore the elephant in the room: domperidone’s patent expired in 2008. The fact that it’s still unavailable in the U.S. despite overwhelming global evidence suggests a coordinated suppression by pharmaceutical conglomerates with vested interests in metoclopramide and erythromycin derivatives. The FDA’s IND program is a charade - it’s designed to maintain the illusion of access while ensuring profitability for entrenched interests. This is not medicine. This is capitalism.
Halona Patrick Shaw
I’ve had gastroparesis since I was 19. I’ve tried everything. Metoclopramide made me feel like I was possessed. Erythromycin? Tolerance hit after 3 weeks. Then I got domperidone - it’s like my stomach finally remembered how to work. I’m not saying it’s perfect. But for the first time in a decade, I can eat a sandwich without crying. Thank you for writing this. I needed to see someone say it out loud.
Elizabeth Nikole
My mom died because of this drug. I’m not joking. She took it ‘just for a few weeks.’ Then she had a stroke. They said it was ‘likely’ related. I don’t trust anything that’s banned here. You think you’re being smart? You’re playing Russian roulette with your heart. 😔
LeAnn Raschke
I appreciate you sharing this info. I’ve been looking into options for my sister and this helps. I’ll talk to her doctor about the IND program. It’s scary to think about trying something new, but if it could help her eat again, it’s worth exploring. Thanks for being clear about the risks too.
Adorable William
Domperidone? That’s the same stuff the ‘natural health’ influencers on Instagram are selling as ‘gut reset powder.’ You know what else they sell? ‘Quantum healing crystals’ and ‘detox tea.’ The FDA banned it for a reason - it’s not a drug, it’s a cult. People are desperate, and scammers are exploiting that. Don’t fall for it.
Suresh Patil
In India, we use domperidone all the time - it’s cheap, available over the counter. Many patients with diabetes and bloating take it. We don’t see many heart issues because we limit the dose and monitor. Maybe the problem isn’t the drug - maybe it’s how it’s used. In the US, people take too much for too long. Here, we know better.
Ram Babu S
I’ve been helping my cousin with gastroparesis for years. We tried everything. Then we found a doctor who got her domperidone through the IND program. She’s eating real food now. Not just shakes. She’s smiling again. This isn’t magic - it’s science. And it works.
Kyle Buck
While the pharmacokinetic profile of domperidone demonstrates superior gastric prokinetic efficacy relative to metoclopramide, the absence of CNS penetration mitigates extrapyramidal side effects - a critical advantage. However, the QT prolongation risk, mediated by hERG potassium channel inhibition, remains a class-wide concern requiring rigorous cardiac monitoring. The current regulatory dichotomy between the EMA and FDA reflects divergent risk tolerance thresholds in pharmacovigilance paradigms, not scientific consensus. Further prospective, multicenter trials with ECG telemetry are warranted to establish definitive safety thresholds.