
Akathisia vs. Restless Legs Syndrome Diagnostic Tool
This tool helps you understand whether your symptoms are more likely to be akathisia or restless legs syndrome (RLS) based on key differences described in the article. This isn't a medical diagnosis, but can help guide your conversation with your doctor.
Symptom Assessment
Medication History
Note: Akathisia is most commonly caused by medications that block dopamine, especially antipsychotics and some antidepressants.
Results
When you can’t sit still-your legs twitch, you pace, you feel like you’re crawling out of your skin-it’s easy to blame stress, anxiety, or just being ‘jittery.’ But what if that restlessness isn’t in your head? What if it’s a direct reaction to a medication you’re taking? Two conditions that look alike but are totally different-akathisia and restless legs syndrome (RLS)-are often confused, and the mistake can be dangerous.
What Is Akathisia, Really?
Akathisia isn’t just fidgeting. It’s a medication-induced movement disorder that makes you feel like you’re being pulled apart from the inside. You don’t want to move because you’re bored-you have to move, or you feel unbearable tension. It’s not voluntary. It’s not anxiety. It’s a physical reaction, usually from drugs that block dopamine in the brain. It most often shows up after starting or increasing a dose of antipsychotics like haloperidol, risperidone, or even some anti-nausea meds like metoclopramide. Symptoms usually appear within days to four weeks. People describe it as an ‘aching restlessness,’ like your bones are buzzing or your skin is too tight. One patient, quoted in a 2017 Australian study, said, ‘I felt like I had to jump out of my skin.’ You’ll notice specific movements: crossing and uncrossing your legs over and over, shifting weight from foot to foot, rocking while seated, or pacing in place. It’s worse when sitting still. Standing or walking helps-but only for a few minutes before the urge comes back.How Is It Different From Restless Legs Syndrome?
Restless legs syndrome (RLS) feels similar, but the trigger and timing are different. RLS strikes mostly at night or during quiet times-when you’re trying to relax or sleep. You get an uncomfortable crawling, tingling, or pulling sensation deep in your legs. Moving helps relieve it, and it usually gets better after you get up and walk around. Akathisia, on the other hand, happens anytime you’re still-especially sitting in a chair or during a doctor’s appointment. It’s not just legs; it’s whole-body agitation. You might feel it in your arms, your torso, your neck. It’s not about discomfort-it’s about an overwhelming, almost panic-like need to move. The biggest clue? Medication timing. If you started a new antipsychotic and two weeks later you can’t sit still, it’s likely akathisia. If you’ve had leg restlessness for years, especially with a family history or low iron, it’s probably RLS. And here’s the kicker: drugs that help RLS-like levodopa or gabapentin-can make akathisia worse. Meanwhile, akathisia often improves with beta-blockers like propranolol or low-dose benzodiazepines like clonazepam, which don’t touch RLS at all.Why Misdiagnosis Is Dangerous
This isn’t just about discomfort. Misdiagnosing akathisia as anxiety or agitation leads to deadly mistakes. In one documented case, a patient on haloperidol developed severe akathisia. His doctor thought he was becoming more psychotic. So they doubled his dose. Within days, he had suicidal thoughts. He didn’t get better until the medication was stopped and clonazepam was added. He was ‘back to himself’ in three days. Studies show up to half of all akathisia cases are misdiagnosed. The American Psychiatric Association warns that untreated akathisia is linked to increased aggression, violence, and suicide risk. Patients have reported choosing to live with untreated psychosis rather than endure akathisia. That’s how bad it gets. Primary care doctors and even some psychiatrists aren’t trained to spot it. They hear ‘I can’t sit still’ and think ‘anxiety.’ They don’t ask about movement patterns. They don’t look for the foot-tapping, the leg-crossing, the pacing. They just prescribe more sedatives-or worse, more antipsychotics.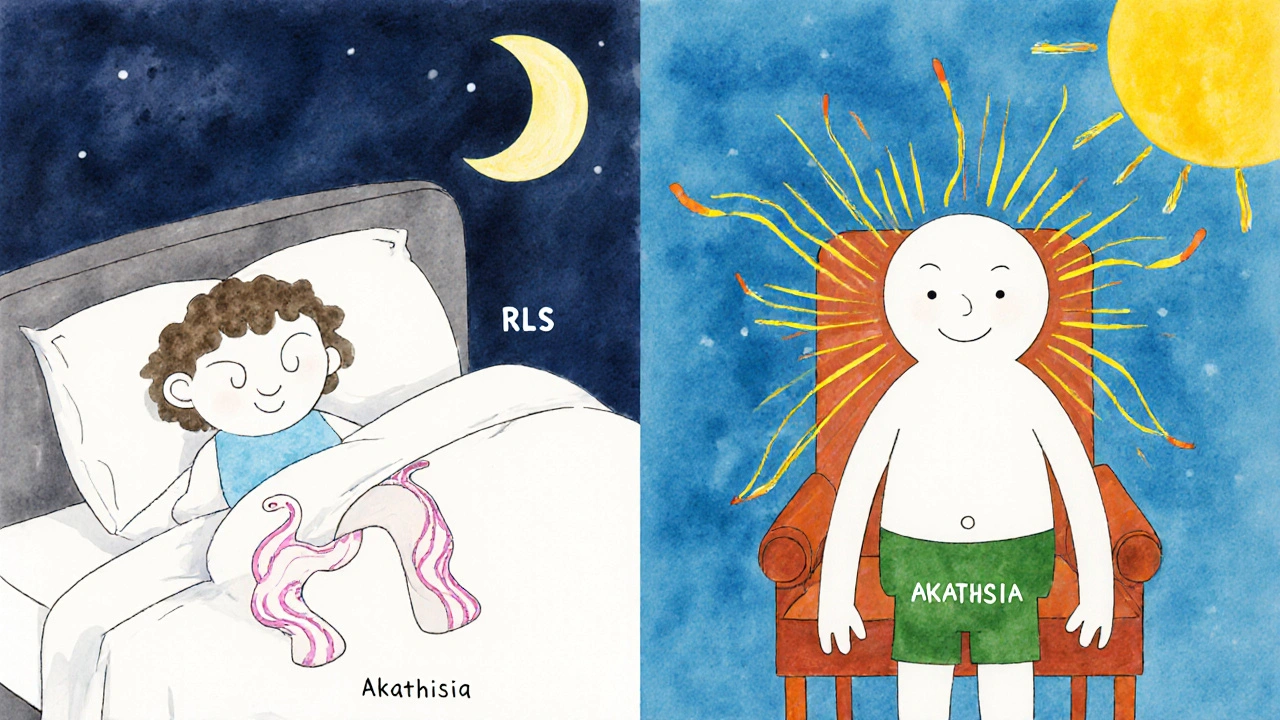
How Doctors Diagnose It
There’s no blood test or brain scan for akathisia. Diagnosis relies on observation and patient history. The gold standard is the Barnes Akathisia Rating Scale (BARS). It’s simple: a clinician asks two questions:- ‘Do you feel an inner sense of restlessness that makes you feel like you must move?’
- ‘Do you notice yourself moving your legs, feet, or body repeatedly without meaning to?’
- Parkinsonism: Tremors, stiffness, slow movements-usually from dopamine blockers, but different from akathisia.
- Tardive dyskinesia: Involuntary lip-smacking, tongue protrusion, or finger movements that happen even when you’re still.
How to Treat It
The best treatment? Stop or reduce the drug causing it. If you’re on haloperidol and have akathisia, tapering the dose over 3-7 days often leads to rapid improvement. In the RACGP case study, symptoms vanished in 72 hours after stopping haloperidol. But sometimes you can’t stop the medication-say, if it’s the only thing keeping psychosis under control. Then you add something to counteract the akathisia. First-line add-ons include:- Propranolol (10-60 mg daily): A beta-blocker that reduces the physical urge to move. Works for many patients.
- Clonazepam (0.5-2 mg nightly): A benzodiazepine that calms the nervous system. Effective, but use cautiously due to sedation and dependency risk.
- Cyproheptadine (4 mg daily): An antihistamine with serotonin-blocking effects. Less commonly used but helpful in some cases.

What You Can Do Right Now
If you’re on an antipsychotic or metoclopramide and you feel restless:- Write down when the restlessness started and what you were taking at the time.
- Track your movements: Do you pace? Cross your legs? Shift constantly? Do it more when sitting?
- Ask yourself: Does this feel like anxiety-or like your body is screaming to move?
- Bring this to your doctor. Say: ‘I think I might have akathisia. Can we check for it?’
- Don’t let them dismiss it as ‘just anxiety.’ Ask: ‘Could this be a side effect of my medication?’
What’s Changing in 2025
Awareness is slowly improving. The International Parkinson and Movement Disorder Society launched a free Akathisia Recognition App in early 2023. It gives clinicians quick checklists and treatment options right on their phone. Research is moving fast. A May 2024 study in JAMA Neurology found unique brainwave patterns in people with akathisia-potentially leading to an EEG-based diagnostic tool soon. New drugs like pimavanserin, originally for Parkinson’s psychosis, showed 62% reduction in akathisia symptoms in a 2023 trial. Non-drug options like transcranial magnetic stimulation are being tested at Harvard and Stanford. But the biggest barrier remains education. Only 37% of U.S. psychiatric clinics routinely screen for akathisia. In Australia, the numbers aren’t much better. Without better training, this condition will keep being missed-and patients will keep suffering.Final Thought: Your Restlessness Matters
If you’ve been told your restlessness is ‘all in your head,’ don’t believe it. Your body is giving you a signal. Akathisia is real. It’s treatable. And it’s not your fault. The right diagnosis can turn a life of torment into a return to normalcy-in days, not years.Can akathisia be caused by antidepressants?
Yes. While antipsychotics are the most common cause, some antidepressants-especially SSRIs like fluoxetine and sertraline-can trigger akathisia, particularly when starting or increasing the dose. It’s less frequent than with antipsychotics, but still reported in up to 10% of patients on high-dose SSRIs. If restlessness starts after beginning an SSRI, akathisia should be considered.
Is akathisia permanent?
Most cases are reversible. Acute akathisia usually clears within days to weeks after stopping or reducing the medication. Chronic akathisia lasts longer than six months and may persist even after stopping the drug, but it’s rare. Tardive akathisia, which appears after long-term use, can be harder to treat, but improvement is still possible with the right approach-like switching medications or adding propranolol.
Can I have both akathisia and restless legs syndrome at the same time?
Yes. Some patients have both. RLS is often linked to iron deficiency or genetics, while akathisia is medication-driven. If you have RLS and start an antipsychotic, you might develop akathisia on top of it. This makes diagnosis harder, but tracking symptom timing helps: RLS is worse at night; akathisia is worse when sitting still during the day. A doctor should check for both.
Why don’t doctors test for akathisia more often?
Most doctors aren’t trained to look for it. Medical school curricula rarely cover movement disorders in depth, and time during appointments is limited. Electronic health records don’t have built-in prompts for akathisia screening. Plus, patients often describe it as ‘anxiety’ or ‘nervousness,’ so the link to medication isn’t made. It’s a systemic blind spot, not a lack of care.
What should I ask my doctor if I suspect akathisia?
Ask: ‘Could my restlessness be caused by my medication?’ ‘Have you ruled out akathisia?’ ‘Can we check the Barnes Akathisia Rating Scale?’ ‘Is there a lower-risk medication I could switch to?’ ‘Would adding propranolol or clonazepam help?’ Don’t accept vague answers. This is a treatable condition-and you deserve to be heard.

Comments (13)
Manish Mehta
Been on risperidone for six months. Started pacing at night. Thought it was stress. Turned out to be akathisia. Stopped the med, switched to lumateperone. Gone in three days. Doctors need to ask better questions.
Okechukwu Uchechukwu
Let me break this down for you. Akathisia isn't a disorder-it's a symptom of pharmaceutical arrogance. The system doesn't want you to know your body is screaming because the drugs are poisoning your dopamine pathways. It's not about treatment-it's about control. They'd rather keep you medicated than admit the cure is stopping the poison.
Renee Williamson
OMG I KNEW IT. My psychiatrist doubled my sertraline and I felt like my bones were vibrating. I screamed at her and left. She called me ‘dramatic.’ Turns out I had akathisia. Now I’m off SSRIs and on a beta-blocker. I cried for three days. I’m alive again. Thank you for this post.
Muzzafar Magray
This is just another way for pharma to sell more drugs. Akathisia? Sounds like people just can’t handle stillness anymore. Maybe try yoga instead of blaming your meds. Everyone’s too addicted to blaming something else for their discomfort.
Sarah Cline
If you’re reading this and you feel like you’re crawling out of your skin-don’t wait. Go to your doctor tomorrow. Bring this article. Say: ‘I think it’s akathisia.’ You deserve to feel normal again. You’re not broken. The drug is.
Khaled El-Sawaf
The author presents a compelling case, yet fails to address the broader ethical implications of prescribing dopamine antagonists without mandatory movement disorder screening. The medical establishment’s institutional negligence in recognizing akathisia constitutes a form of medical malpractice by omission. The fact that half of cases go undiagnosed is not a statistical anomaly-it is a systemic failure.
Nawal Albakri
They’re all lying. The FDA knows this happens and hides it. Look at the black box warnings-they’re buried in 300-page PDFs. Big Pharma pays off the psychiatrists. I’ve seen it. My cousin died because they called his akathisia ‘aggression’ and gave him more antipsychotics. They don’t care. They just want you to keep buying pills.
Musa Aminu
Why are Americans so weak? In Nigeria, we take meds and just move. You think you’re sick because you can’t sit still? We’ve been walking ten miles to clinic with no meds and still no complaints. This is a first-world problem dressed up as a medical crisis.
robert maisha
There is a metaphysical dimension to akathisia. It is not merely neurological but existential. The body rebels against the artificial suppression of the self. The mind is not the self. The urge to move is the soul screaming for liberation from chemical imprisonment. We have forgotten that healing requires surrender, not substitution.
Alexander Ståhlberg
Let me be blunt: if you're on an antipsychotic and you're restless, you're not 'anxious.' You're being poisoned. And if your doctor doesn't know the Barnes scale? They're not qualified to prescribe it. I've seen too many people turned into zombies because someone thought 'fidgeting' meant 'psychosis.' You're not crazy. You're being treated like a lab rat. And that's not just negligence-it's cruelty dressed in white coats.
Robert Andersen
Had RLS since I was 18. Took ropinirole. Then got prescribed sertraline for depression. Two weeks later I couldn't sit in a chair. Thought I was losing my mind. Found this article. Switched to propranolol. Akathisia gone. RLS still there but manageable. Two different things. Don't mix them up.
Megan Oftedal
I’m a nurse. We had a patient on haloperidol who kept getting labeled ‘noncompliant’ because she wouldn’t sit still. She was pacing, rocking, twisting. We finally checked the BARS scale. Turned out she had severe akathisia. We stopped the med, gave her clonazepam, and she cried saying she felt like she’d been trapped in a cage for months. We didn’t even know to look. We’re supposed to help. We failed her.
Sierra Thompson
Medication-induced movement disorders are the silent epidemic nobody talks about. We diagnose depression, anxiety, psychosis-but we ignore the body’s protest. Akathisia isn’t a side effect. It’s a warning. And we’re ignoring the warning signs because it’s easier than admitting our treatments are flawed.